Kids walk up on their toes. Sometimes it is for fun. Other times it is to reach up to grab something, usually something they shouldn’t be! But, there are other potential medical causes of toe-walking as well. Most toe-walking in kids is benign and resolves with just “tincture-of-time.” But, because potential causes of toe-walking fall on a spectrum of varying scariness, it is important for a child who toe-walks to be evaluated carefully.
Causes
A child’s toe-walking typically falls into one of four categories:
- Neuromuscular
- Orthopedic
- Sensory-based
- Idiopathic
Neuromuscular
For the neuromuscular type of toe-walking, it is most often caused by one of many conditions that result in an increase in tone in the calf muscles. This increased tone causes the foot to push down into a toe-walking position involuntarily. Possible causes include but are not limited to cerebral palsy, stroke, brain or spinal cord tumor, and tethered cord. These kids will very often have other challenges such as weakness, poor balance/coordination, or impaired motor control. If the cause is in the spinal cord, bowel and bladder function may be affected as well.
Toe-walking can also be caused by weakness. If the muscles a child depends on to stand and walk are weak, that child may need to use various compensation patterns to support their body. The muscles involved are typically are the ones that extend the hips and knees. Most commonly, the muscular weakness is due to a muscular dystrophy or myopathy. In these conditions, the muscle fibers do not function normally, resulting in the weakness. Depending on the type of muscular dystrophy or myopathy, a child may have weakness from when they were a baby or the weakness may develop later on in life.
Orthopedic
Conditions that result in either shortening of tendons or joints getting “stuck” can result in toe-walking. Because of their positioning in the womb, some babies are born with tight Achilles tendons. The tightness may not be noticed until that child begins to walk. Because of the tightness, the child cannot stand or walk with their feet flat on the ground. In other cases, a person who spends a considerable amount of time with the ankles in the “toes-down” position can develop tightness in the Achilles tendon or ankle joint itself. This may occur when one has an injury and spends a few weeks in bed. But, even a change to a more sedentary lifestyle can result in this type of tightness developing. I’ve seen kids during the COVID-19 pandemic with remote learning spend so much more time doing their schoolwork and recreational activities sitting or lying down, they developed Achilles tendon tightness that they starting toe-walking! In some cases, the decreased activity was enough to cause enough Achilles tendon tightness to result in toe-walking!
Sensory-Based
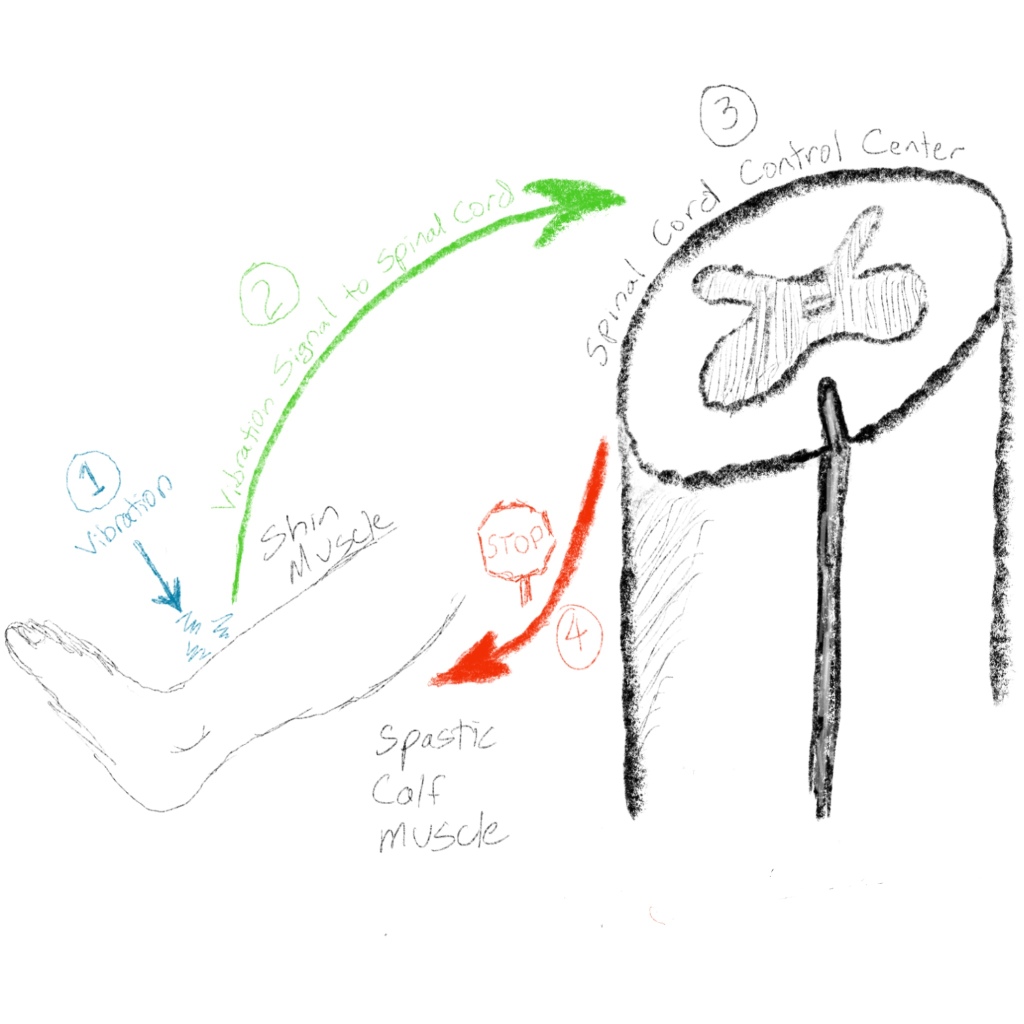
Children with Sensory Integration Disorder can be “sensory-defensive” or “sensory-seeking,” both of which can cause toe-walking. That’s a bit confusing because sensory-defensive and sensory-seeking appear to be opposites! Sensory-defensive kids toe-walking because they are adverse to the feeling of the floor on the bottom of their feet. They rise up on their toes to minimize the contact of the very sensitive soles of their feet and the ground, especially on cold or rough surfaces. Kids who are sensory-seeking rise up on their toes to increase sensory input from the various sensors in the muscles of the feet and legs. These include position, stretch vibration, and other sensors. By rising up on their toes, they put themselves in an unstable position where the body needs more input from these sensors to balance and stay stable. They may even have a little bounce in their steps to increase this sensory input. This increased sensory input feeds their sensory-seeking needs. Toe-walking is more common in children with Autism than in children without Autism. Most children with Autism who are toe-walkers do so for sensory reasons.
Idiopathic
“Idiopathic” refers to conditions where the cause is not known. It is often a diagnosis of exclusion where all other causes are “ruled out.” Though the kids with idiopathic toe-walking, don’t have a neuromuscular, orthopedic, or sensory cause of their toe-walking, it is not unusual to have relatives who are also toe-walkers, suggesting a genetic cause.
Most kids with idiopathic toe-walking start walking on their toes as soon as they learn to walk. Most of them stop toe-walking after a few years without any specific treatment. However, some kids with idiopathic toe-walking become adults who walk on their toes. Often, this happens because that individual would have stopped toe-walking at some point during childhood; but, they couldn’t because they had already developed Achilles tendon contracture, resulting in this physical barrier to the stopping of the toe-walking. For this reason, even though idiopathic toe walking isn’t due to an underlying medical cause, and most idiopathic toe-walkers stop on their own, treatment may still be needed.
Treatments
There are numerous treatments for toe-walking. But, for success, the correct combination of treatments for each individual needs to be established. I’ll touch upon some of them here.
Braces (Orthoses)
The most common brace used to treat toe-walking is the ankle-foot-orthosis (AFO). AFO’s are plastic (or sometimes carbon fiber), custom-molded braces that extend from the feet to the upper calf. For toe-walking, they should almost always have a hinge at the ankle that allows for the foot to dorsiflex (point up), but prevents the foot from plantar-flexing (point down) past neutral. AFOs help in a couple of ways. By preventing the foot from plantar-flexing past neutral, it mechanically prevents that child from toe-walking. By preventing toe-walking, the AFOs can help that child to “internalize” a regular heel-toe walking pattern. They also help by preventing or slowing down the worsening of the Achilles tendon tightness.
Nighttime dorsiflexion splints can also help to maintain the flexibility at the ankle. When we sleep, whether we do so on our backs, sides, or belly, our ankles are almost always in a toe-down position. Being in this position for the several hours of sleep results in worsening of the ankle tightness. By using a nighttime splint, similar to an AFO, worsening tightness can be prevented or slowed. Of course, this requires a child to be a pretty sound sleeper! If wearing nighttime splints prevents the child from getting a good night’s sleep, they aren’t worth it!
Therapies
Both physical and occupational therapy can be helpful. A physical therapist can help to teach some toe-walking children to walk in a more heel-toe pattern. They can also help to stretch the tight muscles as well as teach the child and/or family members to stretch at home. Physical therapy homework is very important! A physical therapist may also be trained in other techniques that may be helpful such as Kinesiotaping. I’ll have to cover the topic of Kinesiotaping in another post. It’s a big one! In the situation of toe-walking caused by a neuromuscular or orthopedic cause, the physical therapist would treat the toe-walking in the context of the comprehensive physical therapy treatment of the underlying condition.
For kids who toe-walk for sensory reasons, occupational therapists are often an essential component of the team. Toe-walking due to sensory reasons is extremely difficult to stop while the sensory integration issues are still impacting that child.
Serial Casting
Serial casting is a technique that is very helpful for stretching tight muscles. It is most often provided by specially-trained physical therapists. Sometimes pediatric orthopedic surgeons perform it. In serial casting for tight Achilles tendons, therapist of orthopedist stretches the ankle in the up-position and applies a lightweight cast, similar to one that would be used for a broken bone. That child would then keep the cast on for one to two weeks, carrying on as usual. Walking is encouraged during this time. After one to two weeks, the cast is removed and the ankle is stretched further. With each cast, the ankle joint should get more flexible. These steps are repeated until the goal range is reached or the casts aren’t resulting in increased range-of-motion. Most kids tolerate the casts better than expected. But, warm weather, especially if a child enjoys swimming, is not a great time to serial cast since the casts cannot get wet.
Botulinum Toxin (Botox) Injections and Alcohol/Phenol Nerve Blocks
Botox and nerve blocks are injection procedures that reduce the “hyperactivity” of muscles by blocking some of the signals traveling between the muscle and the nerve that “controls” it. In kids who toe-walk due to “spasticity” from an injury to the brain or spinal cord, these injections can be very effective in reducing the involuntary contraction of these muscles that is causing the toe-walking. For these kids, the injections need careful planning in a comprehensive way that takes into account all of the other neuromuscular effects of that medical condition. These injections can also be helpful for idiopathic and sensory-based toe-walkers by weakening the calf muscles so it is more difficult for those children to rise up on their toes. During the period of time that the injections are in effect, the flatter walking pattern can be better “internalized” and worsening of the contractures can be prevented.
One of the most commonly mentioned disadvantages of Botox and nerve blocks is that they are temporary. Botox typically lasts for three to six months. Nerve blocks typically last six months or more. However, one of the major advantages of these injections is that they are temporary! Since kids are changing so quickly during growth and development, the factors causing their toe-walking are also changing. A temporary treatment like Botox and nerve blocks allow for better tailoring and adjusting of the treatment to meet the needs of each individual over time.
Botox injections and nerve blocks are most commonly performed by Pediatric Physiatrists (physicians who specialized in Physical Medicine and Rehabilitation Medicine). Neurologists and orthopedists also sometimes perform them.
Orthopedic Surgery
If an Achilles tendon gets too tight, serial casting and other more conservative treatments may not be enough. An orthopedic surgeon can lengthen a tendon using several different surgical techniques. The recovery time as well as how much flexibility can be gained varies with the different techniques. For this type of surgery to be successful (and not cause worsening of the walking), it should be performed by a pediatric orthopedic surgeon experienced in these techniques, with planning and decision-making performed together with the patient, family, and entire treatment team.
Recap
There are a lot of kids out there walking on their toes. Most will do just fine and will stop toe-walking on their own. But, since there are some scarier causes of toe-walking, an evaluation by a Pediatric Physiatrist should certainly be considered. And, even if the toe-walking is idiopathic, treatment is sometimes still needed for those kids who get tight at a young age or continue to toe-walk past the toddler years.